

Introduction:
There is currently no consensus on the optimal frontline therapy for patients with T cell Non-Hodgkin lymphomas (T-NHL). Consolidative autologous stem cell transplant (ASCT) is frequently offered to the patients with chemosensitive disease based on retrospective and prospective studies showing improved progression-free survival (PFS) when compared with historical controls getting chemotherapy alone. However, it remains unclear whether there is a good risk subset of patients who achieve first complete remission (CR1) following induction chemotherapy and who might not benefit from upfront ASCT. To date, no randomized control trials (RCTs) exist and available data is conflicting. We perform a systematic review/meta-analysis of the published literature to address this question.
Methods
A comprehensive, systematic search (from database inception - 9/2019) of MEDLINE/PubMed, EMBASE and Cochrane databases was performed. PRISMA and Meta‐Analysis Of Observational Studies in Epidemiology (MOOSE) guidelines were followed. Studies were selected from a total of 2656, screened based on predefined inclusion/exclusion criteria, and were critically appraised for outcomes of interest [progression free survival (PFS) and overall survival (OS)]. Quality of studies was assessed using Newcastle-Ottawa Scale. Hazard ratios (HRs) and corresponding 95% Cis were calculated, and the meta-analysis was performed using the random-effects model. Test for heterogeneity was performed using I2 statistic.
Results
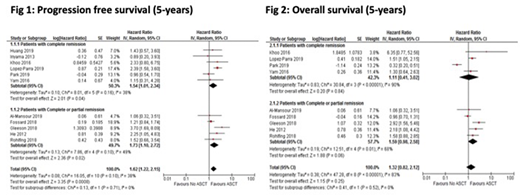
Of 2656 unique records, 13 studies (prospective = 3; retrospective = 10) were selected. In 8 studies, upfront ASCT was compared to NO ASCT in patients in first complete remission (CR1), while in 5, comparison was with patients achieving either PR1 (first partial remission) or CR1. 11 (of 13) studies reported PFS. Median follow-up in these studies ranged from 22 months to 7.8 years. Results from the meta-analysis showed that T-NHL patients who underwent ASCT had an improved 5-year PFS compared to those with NO ASCT (HR 1.62, 95% confidence interval (CI) 1.22 to 2.15, I² = 38%) (Figure 1). However, no benefit was observed in 5-year OS when ASCT was compared to NO ASCT (HR 1.32, 95% CI 0.82 to 2.12, I2 = 83%) (Figure 2). A sensitivity analysis including only studies with patients transplanted in CR1 showed similar findings, with a 5-year PFS (HR 1.54, 95% confidence interval (CI) 1.01 to 2.34, I² = 38%) and 5-yr OS (HR 1.11, 95% CI 0.41 to 3.02, I2 = 90%) when compared to No ASCT.
Conclusions
In the absence of RCTs, the results of this systematic review/meta-analysis represents the best evidence supporting long term PFS benefits of upfront ASCT consolidation in patients with T-NHL in CR1 or CR1/PR1 after frontline chemotherapy.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal